AMA Announces Major Overhaul of Maternity Care CPT Codes Beginning in 2027
Quick Answer
Effective January 1, 2027, the AMA is replacing the decades-old global obstetric CPT billing model with a four-phase, service-level framework covering antepartum, labor management, delivery, and postpartum care. The overhaul — the largest restructuring of maternity coding in over 30 years — eliminates 17 existing codes, adds 12 new ones, and revises 6 others, directly affecting every OB/GYN practice, certified nurse midwife, and maternity billing team in the country.
Why Is the AMA Overhauling Maternity CPT Codes in 2027?
If you’ve been billing obstetric services for more than a few years, you know the global OB package inside and out. One code. Nine months of care. Clean and simple — at least on paper.
But that simplicity has been quietly misrepresenting how maternity care actually gets delivered for decades.
The Current Procedural Terminology (CPT) Editorial Panel has approved a significant restructuring of maternity care services codes for the CPT 2027 code set. Effective January 1, 2027, CPT codes will better reflect modern obstetric practice, enable accurate and transparent reporting across the full pregnancy spectrum, and create the data foundation necessary to better attribute maternal care and support the complexities of team-based care throughout a patient’s journey.
More provider types are now involved in maternity care, such as certified nurse midwives, laborists, and postpartum specialists, and the care they provide is often more complex than what the global codes include. Patients are also more likely to bounce between different sites of service, like high-risk patients being transferred from rural hospitals to better-equipped facilities. Such transitions are difficult to capture under global codes.
The honest assessment from someone who has watched billing workflows in OB practices: the global code was never a clinical description. It was an administrative convenience. And it worked reasonably well when one physician managed a pregnancy from first prenatal visit to six-week postpartum check. That model of care is largely gone. The new code structure finally acknowledges that.
The AMA’s CPT Editorial Panel approved an overhaul to the maternity codes during its September 2025 meeting. The announcement was formally published by ACOG on April 23, 2026, giving practices slightly under nine months to prepare before the January 1, 2027 implementation date.
What Exactly Is Changing Under the CPT 2027 Maternity Code Overhaul?
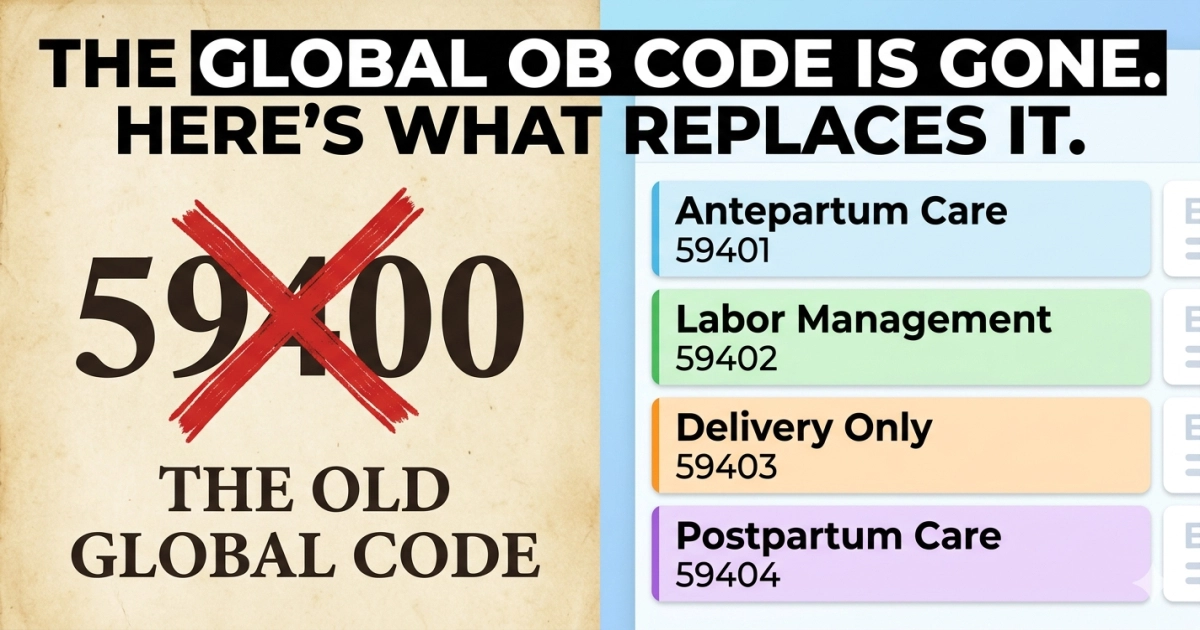
The End of the Global OB Package
For OB/GYN billing teams, this is not a minor update. The AMA Editorial Panel has approved a complete overhaul effective January 1, 2027. The global OB package model is gone. In its place, every phase of pregnancy care is billed separately. That shift touches every coder, biller, and practice manager working in this specialty.
In total, 35 codes were changed: 17 deleted codes, 12 new codes, and 6 revised codes. The traditional global maternity codes will be deleted and replaced with phase-specific reporting.
Among the deleted codes are some of the most commonly reported in OB/GYN billing history:
17 existing maternity codes will be deleted, including: 59400 — Routine obstetric care including antepartum care, vaginal delivery (with or without episiotomy, and/or forceps) and postpartum care.
Global antepartum-only codes 59425 and 59426 and the antepartum portions of all full global codes (59400, 59510, 59610, 59618) will be deleted or substantially restructured.
The Four New Phases of Reporting
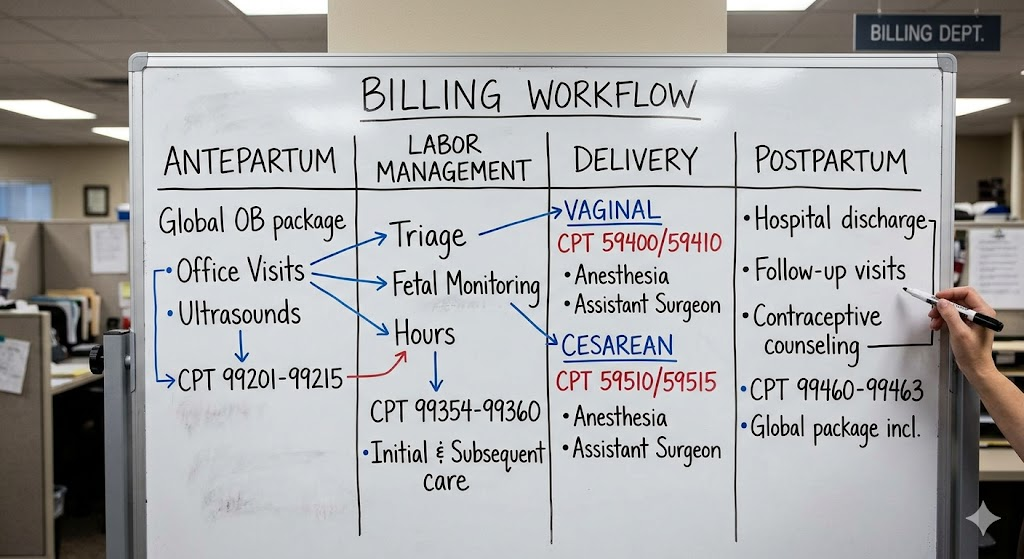
Beginning January 1, 2027, care will be reported more granularly at the service level, separately identifying four phases of care: antepartum, labor management, delivery, and postpartum. The delivery of maternity care has changed fundamentally over the past three decades. Pregnancy care is now routinely delivered by multiple, sometimes unaffiliated care teams across all phases. Patients are frequently transferred from rural hospitals to facilities equipped to manage higher-risk obstetric and neonatal cases, and today’s bundled codes do not adequately reflect that care.
Here’s how each phase now works:
Phase 1 — Antepartum Care
Antepartum care will now be reported per encounter using Evaluation and Management (E/M) services. As with other E/M services, the specific code reported for a given encounter will be based on either total time on the date of the encounter, or medical decision making (MDM). The 2027 revisions do not assign a fixed level of complexity to a given patient across all antepartum encounters.
ACOG recommends that health plans begin the transition from the global obstetric payment by using the E/M codes (CPT 99202–99499) without limitations or preauthorization requirements for antepartum visits no later than September 1, 2026. It is recommended that the HCPCS modifier “TH” be appended to the E/M code to differentiate the visit as maternity care.
Phase 2 — Labor Management
Labor management will now be reported daily, with additional codes for initial and subsequent days, and codes for labor management will be separated from delivery care.
Four new codes will distinguish labor management based on the day and complexity: 59XX1 (Initial day, straightforward), 59XX2 (Initial day, complex), 59XX3 (Subsequent day, straightforward), and 59XX4 (Subsequent day, complex).
Labor management will include interim physical examinations, collection and interpretation of physiological data, and collection and interpretation of monitoring data.
Phase 3 — Delivery Care
Starting in 2027, delivery care codes will not be dependent on who performs the delivery or whether the patient is getting a vaginal birth after cesarean (VBAC). Codes for attempted VBAC after cesarean that led to a cesarean were not carried over. The rationale was that the work for increased complexity would be captured under the new labor management codes.
Phase 4 — Postpartum Care
All current postpartum care codes will be deleted and reported per encounter with E/M codes in 2027. Routine postpartum care on the same calendar day as the delivery is incorporated separately.
All current postpartum care codes will be deleted, including the standalone 59430. For facility births, providers will use appropriate subsequent hospital care codes for each management day. Outpatient E/M services (99212–99215) will be used for postpartum care after discharge.
What Does This Mean for Reimbursement — Will Practices Make More or Less?
This is the question every OB/GYN practice manager is asking right now, and the honest answer is: it depends on how prepared you are.
At a national policy level, CMS and the AMA have been clear: the CPT 2027 maternity care revisions are expected to be budget neutral. Survey data from more than 650 obstetricians, family physicians, and certified nurse midwives were used by the RVS Update Committee (RUC) to assess physician time, intensity, and complexity. The resulting work RVU recommendations were structured so that, in aggregate, total RVUs generated under the new code set do not exceed those produced by the former global maternity codes.
But “budget neutral” is a system-level projection. It does not mean every practice breaks even.
Budget neutrality at the system level does not translate into neutral impact for individual clinicians or practices. The new structure redistributes revenue based on how care is delivered, how frequently patients are seen, and how well practices adapt documentation, coding, and workflow. As a result, some obstetricians may experience improved revenue capture, while others could see downward pressure if operational changes are not made.
Practices that stand to gain the most are those operating in high-acuity, team-based environments where multiple providers contribute to care across phases. Practices with leaner structures handling lower-risk, single-provider pregnancies may need to be more deliberate about documentation to maintain prior revenue levels.
While final CMS RVU values will not be published until late 2026, the trajectory is clear. Practices that engage early in education, workflow redesign, and E/M optimization will be best positioned to adapt to the new payment model and minimize unintended financial disruption.
One pattern worth watching closely: because antepartum visits will now generate individual E/M claims rather than folding into a global bundle, payers will gain real-time visibility into their members’ pregnancies earlier in the episode. That’s a meaningful shift — and one that billing teams should anticipate triggering more utilization review and preauthorization scrutiny on complex cases.

How Does This Affect Certified Nurse Midwives and Non-Physician Providers?
The CPT changes affect attribution — how work is recognized and credited — not workload. Care has become more complex, often involving teams of clinicians, including laborists, certified nurse midwives, advanced practice providers, and postpartum specialists. These clinicians work across the different phases of the maternity episode and sometimes across multiple care sites.
Under the old global model, a CNM who managed labor but didn’t perform the delivery was largely invisible in the billing record. Their work was absorbed into a global package billed by another provider. The new structure changes that significantly — every clinician performing a distinct phase of billable care can report it separately under their own provider identification.
The new framework allows providers to document and bill for each service rendered, ensuring continuity and transparency. Modern obstetric care includes a wide range of services beyond traditional visits, including screenings for mental health and social determinants, genetic counseling, nutrition counseling, and patient education for self-monitoring.
For midwife-led practices, this is potentially significant. If your scope includes antepartum management, labor management, or postpartum care delivered as distinct encounters, you now have dedicated reporting pathways that didn’t exist cleanly before.
Two Insights From Coding and Billing Professionals in the Field
On the documentation bottleneck: A recurring concern among experienced OB coders is that the new system places enormous weight on real-time, accurate clinical documentation. Under the old global model, documentation gaps were often absorbed without direct financial consequence — the global code got billed regardless. Under the new phase-specific model, every encounter needs to independently support the E/M level or specialty code being reported. Practices that haven’t invested in documentation training for their clinical staff are going to feel this gap immediately in 2027. The coding team can only report what the provider has documented. If the documentation doesn’t support a 99214 for that antepartum visit, the coder has to downcode — and that revenue doesn’t come back.
On payer contract renegotiation timing: Revenue cycle managers who have been through major CPT restructuring before are pointing out something practices may be overlooking: existing payer contracts may contain language that specifically references deleted global codes. If your fee schedules reference 59400 or 59510, those contracts may need to be renegotiated before January 1, 2027, or you could face claim denials simply because the contractual billing reference no longer exists. The CPT Editorial Panel chose to release the new maternity codes for 2027 early given the mammoth task of implementation. It could take insurers and their vendor partners months to pivot to the new maternity codes, given how deeply the current global codes are woven into healthcare reporting and billing systems. That early release is your window. Use it now to contact payers about contract language, not in December.
How Should OB/GYN Practices Prepare for the January 2027 Transition?
You have less than seven months from the April 2026 announcement to get your entire revenue cycle aligned with a completely new billing structure. That sounds like a long time. It isn’t.
Here’s where to focus first:
Audit your current workflow against the four new phases. Map out which providers in your practice deliver care in each phase. Understand who currently gets attributed in billing and who doesn’t. This gap analysis will reveal both revenue recovery opportunities and documentation risks.
Train clinical staff on E/M documentation standards for antepartum and postpartum. Because both phases now use E/M coding rules, providers need to understand how to document medical decision making or time in a way that supports the appropriate E/M level. This is not just a coding problem — it’s a clinical documentation problem.
Contact your payers now — not in November. Codes 59425 and 59426 will be available in 2026 but will be deleted in 2027. ACOG recommends that health plans begin the transition to E/M codes for antepartum visits no later than September 1, 2026, to avoid undue administrative burdens and incorrect billing. If your payer hasn’t started transitioning yet, start that conversation immediately.
Update your practice management software. Every EHR and billing platform that touches OB/GYN claims will need to be updated for the new code set. Confirm with your vendor that they have a 2027 CPT update roadmap and a go-live timeline that leaves time for testing before January 1.
Review and revise your fee schedules. Once the final CPT 2027 code set is published with RVU values in late 2026, update your internal fee schedules to reflect the new codes. Don’t wait until January to discover mismatches.
What Resources and Training Are Available Right Now?
To help the health care ecosystem prepare to implement these revisions and enable physicians to deliver the best care possible to their patients, the AMA is developing educational resources to support the health care ecosystem.
The AMA has published its CPT 2027 Maternity Care Services FAQ and downloadable code change list directly at ama-assn.org, which is the authoritative first stop for any practice beginning its transition planning. ACOG has also published guidance at acog.org, including payer transition recommendations and modifier usage guidance.
Phase-specific reporting provides earlier visibility into specific care provided, facilitates early detection of pregnancy risks via frequent E/M claims and ICD-10 diagnoses (e.g., medical complexity, social determinants of health), and highlights key information to identify beneficial interventions.
For practices that want hands-on support, revenue cycle management firms specializing in OB/GYN and Maternal-Fetal Medicine are actively developing 2027-specific implementation services. This is one area where outsourcing the transition planning — or at minimum getting a revenue cycle audit before year-end — can pay for itself quickly.
FAQ
The revisions will take effect starting January 1, 2027, and pertain to billing for maternity care services including prenatal care, labor and delivery, and postpartum care. Practices cannot use the deleted global codes for services rendered on or after that date.
35 total codes were changed, including 17 deleted codes, 12 new codes, and 6 revised codes.
The CPT 2027 maternity care revisions are expected to be budget neutral at the system level. However, budget neutrality does not translate into neutral impact for individual clinicians or practices. The new structure redistributes revenue based on how care is delivered, how frequently patients are seen, and how well practices adapt documentation, coding, and workflow.
It is recommended that the HCPCS modifier “TH” be appended to the E/M code to differentiate the visit as maternity care. This helps payers correctly attribute the encounter to the pregnancy episode rather than treating it as a standalone E/M visit.
Survey data from more than 650 obstetricians, family physicians, and certified nurse midwives were used by the RUC to assess physician time, intensity, and complexity in developing the new RVU recommendations. CNMs who provide distinct phases of care will now have dedicated reporting pathways to bill their services separately under their own NPI, improving attribution accuracy for team-based care models.
Immediately. ACOG recommends that health plans begin the transition to E/M codes for antepartum visits no later than September 1, 2026, to avoid undue administrative burdens and incorrect billing. Payer system updates and contract reviews take time — starting in the fall of 2026 is too late for many organizations.
Codes for attempted VBAC after cesarean that led to a cesarean were not carried over to the new code set. The rationale was that the work for increased complexity would be captured under the new labor management codes.
The AMA has published the complete downloadable code change list at ama-assn.org/practice-management/cpt/cpt-2027-maternity-care-services-code-changes. ACOG’s coding library at acog.org also provides complementary payer guidance and transition recommendations.
References
- American Medical Association — “CPT 2027 Maternity Care Services code changes.” ama-assn.org/practice-management/cpt/cpt-2027-maternity-care-services-code-changes (Published April 22, 2026)
- American Medical Association — “FAQs: CPT 2027 Maternity Care Services code changes.” ama-assn.org/practice-management/cpt/faqs-cpt-2027-maternity-care-services-code-changes
- American College of Obstetricians and Gynecologists — “Payment for Obstetric Services – Coding.” acog.org/practice-management/coding/coding-library/payment-for-obstetric-services
- Healthcare Dive — “AMA creates new maternity care coding system.” healthcaredive.com/news/ama-maternity-code-overhaul-pregnancy-obgyn-cpt/813363 (March 2, 2026)
- The Cardiology Advisor / Endocrinology Advisor — “AMA Updates Maternity Care Service Codes for 2027.” thecardiologyadvisor.com (April 28, 2026)
- MedCentral — “New OB Coding Rules May Expand Revenue — But Expect Closer Scrutiny.” medcentral.com (April 29, 2026)
- The ObG Project — “The New 2027 Maternity Care Codes: What to Know About Reimbursement Impact.” obgproject.com (April 23, 2026)
- Kovor Revenue Cycle Management — “Navigating the 2027 CPT Maternity Care Overhaul: Implications for OB/GYN and Maternal-Fetal Medicine Revenue Cycle Management.” kovorcm.com (March 31, 2026)
- Transcure — “Maternity Care Coding Updates 2027: Complete Guide for OB/GYN Billing.” transcure.net
- Coker Group — “The Shift That Changes Everything: Understanding the 2027 Maternity Coding Changes.” cokergroup.com (April 14, 2026)
Author Bio
Dana R. is a certified medical billing and coding specialist with over 12 years of experience in OB/GYN and Maternal-Fetal Medicine revenue cycle management. She has overseen billing compliance for multi-provider obstetric practices through multiple CPT and ICD-10 transitions, and currently consults with practices preparing for the 2027 maternity coding overhaul. Dana writes to help coders and practice managers cut through policy documents and understand what changes actually mean for daily workflows and financial performance. All content is for educational purposes. Practices should consult qualified legal and compliance counsel for situation-specific guidance.
Compliance Disclaimer: CPT codes and billing guidance described in this article reflect publicly available AMA and ACOG documentation as of June 2026. Final RVU values and complete code descriptors for CPT 2027 will be published by the AMA in late 2026. Practices should verify all code selections and billing guidance against final published materials prior to implementation.